

What is a Capitate Fracture?
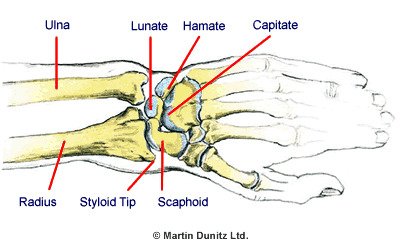
A broken wrist commonly occurs following a fall on an outstretched hand. A capitate fracture accounts for around 2% of all wrist fractures. The capitate is one of the eight small carpal bones that make up the wrist complex. It is positioned in the centre of the carpal region and is therefore quite well protected. Isolated capitate fractures can occur but, more often, capitate fractures occur together with fractures of another carpal bone – the scaphoid. These injuries usually occur following a fall onto an outstretched hand.
Signs & Symptoms of a Capitate Fracture
There is a good deal of wrist pain and tenderness at the back of the wrist. Moving the hand back (wrist extension) will exacerbate the pain.
In the first 48 hours following injury, a capitate fracture is difficult to detect on x-ray and can often be missed in the early stages. A cautious approach should therefore be taken. Supporting the wrist in a protective brace can be helpful to relieve pain and protect against too much movement. If the wrist is still painful after two weeks the wrist should be x-rayed again. At this stage the fracture is more easily visible on the x-ray.
Because the capitate has a poor blood supply there are sometimes complications with the healing process. This may manifest itself as a diffuse ache in the wrist upon activity, and can persist for many months. This is due to a breakdown of the capitate caused by the lack of blood supply and healing (avascular necrosis). If these symptoms persist for more than six weeks it is likely that the bone hasn’t healed and the patient should return to the treating doctor.
Treatment for a Capitate Fracture
- Consult a health professional
- Wear a removable cast for protection
- Regain dexterity with therapeutic putty
- Relieve wrist stiffness with hand therapy balls
- Improve finger & grip strength with resistance exercises
- Use a bone healing system to speed up broken bone healing
In the case of an acute capitate fracture where there is x-ray evidence of excellent alignment of the fracture fragments, the attending doctor will immobilise the wrist in a plaster or lightweight wrist brace. This will be worn for a period of 6 weeks to allow healing of the bone to take place. Once the cast has been removed the patient begins physiotherapy treatment to regain range of movement of the wrist joint and strength in the muscles that work over the wrist and elbow.
Rehabilitation begins immediately by maintaining the range of movement in the shoulder, elbow, fingers and thumb, on the side of the affected wrist. This prevents secondary stiffness in these areas and helps to resolve swelling in the wrist. Assuming that there are no complications with healing, the plaster can usually be removed after 6 weeks, if the doctor is satisfied that the bone has united and healed itself. At this stage more active rehabilitation can be undertaken.
Exercises in warm water are helpful to improve the hydration of the skin if it was previously encased in a plaster cast. The buoyancy of the water helps to encourage the patient to gently begin move the wrist in all directions, relieving stiffness. These also encourage the patient to gently begin moving the wrist in all directions, relieving stiffness. Exercises using therapeutic putty, hand therapy balls and grip strengtheners can add strength to the muscles around the wrist and resolve wrist swelling. In the period following the removal of the plaster it may be helpful to wear a supportive splint when not doing the exercises. If regularly desk work, typing, hairdressing or other hand-dominant occupations are undergone continued use of a wrist splint may help when returning to work or activity.
If x-rays show that the capitate fracture fragments are out of alignment by more than 1mm, or that the break is not healing, it may be necessary to treat the problem with surgery. The surgeon uses small screws to unite the two pieces of bone. Often the ligament between the capitate and the scaphoid bone is also injured and this will be repaired at the same time.
Following surgery, a removable plastic cast can provide the same degree of protection as a conventional plaster, but is much lighter and therefore more comfortable to wear. The fact that they can be removed allows washing of the wrist region, making it much more hygienic than a conventional plaster, which allows the user to keep the skin in good condition. Once the treating doctor indicates that the cast is no longer required, physiotherapy treatment can help to restore hand and wrist function. Hand therapy exercises can add strength to the muscles around the wrist, reversing the wasting (atrophy) that occurs during immobilisation and resolve wrist swelling.
Broken Wrist Prevention
There is not a lot that can be done about a fall on an outstretched hand in most sports. However, in snowboarding the incidence of wrist fractures is so high that wrist guards should be worn. They significantly reduce the incidence of wrist injuries during falls and are available from all good ski shops.